Repetitive strain injuries (RSIs) are “injuries of the musculoskeletal and nervous systems that may be caused by repetitive tasks, forceful exertions, vibrations, mechanical compression (pressing against hard surfaces), or sustained or awkward positions”. RSI is also known as cumulative trauma disorders, repetitive stress injuries, repetitive motion injuries or disorders, musculoskeletal disorders, and [occupational] overuse syndromes.
Repetitive strain injury (RSI) is a syndrome incorporating several discrete conditions associated with activity-related arm pain such as edema, tendinitis, carpal tunnel syndrome, cubital tunnel syndrome, thoracic outlet syndrome, stenosing tenosynovitis, intersection syndrome, golfer’s elbow or medial epicondylitis, tennis elbow or lateral epicondylitis, radial tunnel syndrome, and focal dystonia.
Doctors have recently begun making a distinction between tendinitis and tendinosis in RSI injuries. There are significant differences in treatment between the two, for instance in the use of anti-inflammatory medicines, but they often present similar symptoms at first glance and so can easily be confused.
The following complaints are typical in patients who might receive a diagnosis of RSI:
- Short bursts of pain in the arm, back, shoulders, wrists, hands, or thumbs (typically diffuse – i.e. spread over many areas).
- The pain is worse with activity.
- Weakness, lack of endurance.
Treatment
RSIs are assessed using a number of objective clinical measures. These include effort-based tests such as grip and pinch strength, diagnostic tests such as Finkelstein’s test for Dequervain’s tendinitis, Phalen’s Contortion, Tinel’s Percussion for carpal tunnel syndrome, and nerve conduction velocity tests that show nerve compression in the wrist. Various imaging techniques can also be used to show nerve compression such as x-ray for the wrist, and MRI for the thoracic outlet and cervico-brachial areas.
The most-often prescribed treatments for early-stage RSIs include drug therapies such as anti-inflammatory medications combined with passive forms of Physiotherapy such as rest, splinting, massage, mobilisation, taping, acupuncture. Low-grade RSIs can sometimes resolve themselves if treatments begin shortly after the onset of symptoms. However, some RSIs may require more aggressive intervention including surgery and can persist for years.
General exercise has been shown to decrease the risk of developing RSI. Doctors sometimes recommend that RSI sufferers engage in specific Physiotherapy guided strengthening exercises, for example to improve sitting posture, reduce excessive kyphosis, and potentially thoracic outlet syndrome.
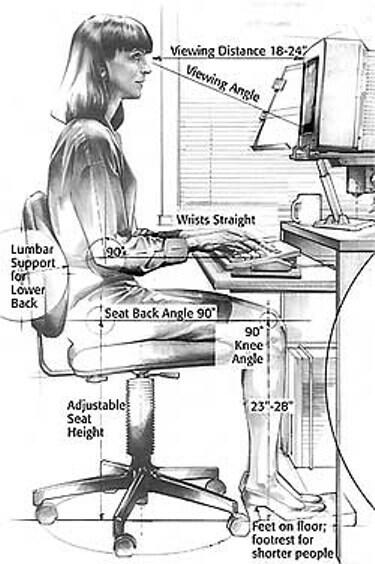
Since workstation design often contributes to RSIs, ergonomic adjustments of the workstations are often recommended.